General Details:
32 years old married female
Therapeutic Mammoplasty With Sentinel Node
General Details:
32 years old married female
Symptoms/ Signs:
Lump in Left Breast since 15 days
Examination:
Definite single and palpable hard mass 2 cms in size in upper outer quadrant of left breast
No skin or nipple changes
No axillary lymph nodes
History:
No significant medical or gynaecologic or family history
Menstrual H/o – Normal
Diagnostics:
Cluster of branching microcalcifications seen in lower inner quadrant of left breast.
Findings s/o high grade DCIS with comedo necrosis. BIRADS IV lesion.
24x16mm hypoechoic lesion with multiple tiny calcifications at 9’o clock position
Management:
Surgery: Left Breast Wide Local Excision with Therapeutic Mammoplasty with Sentinel Node Biopsy with Right Side Reduction Mammoplasty
Discussion:
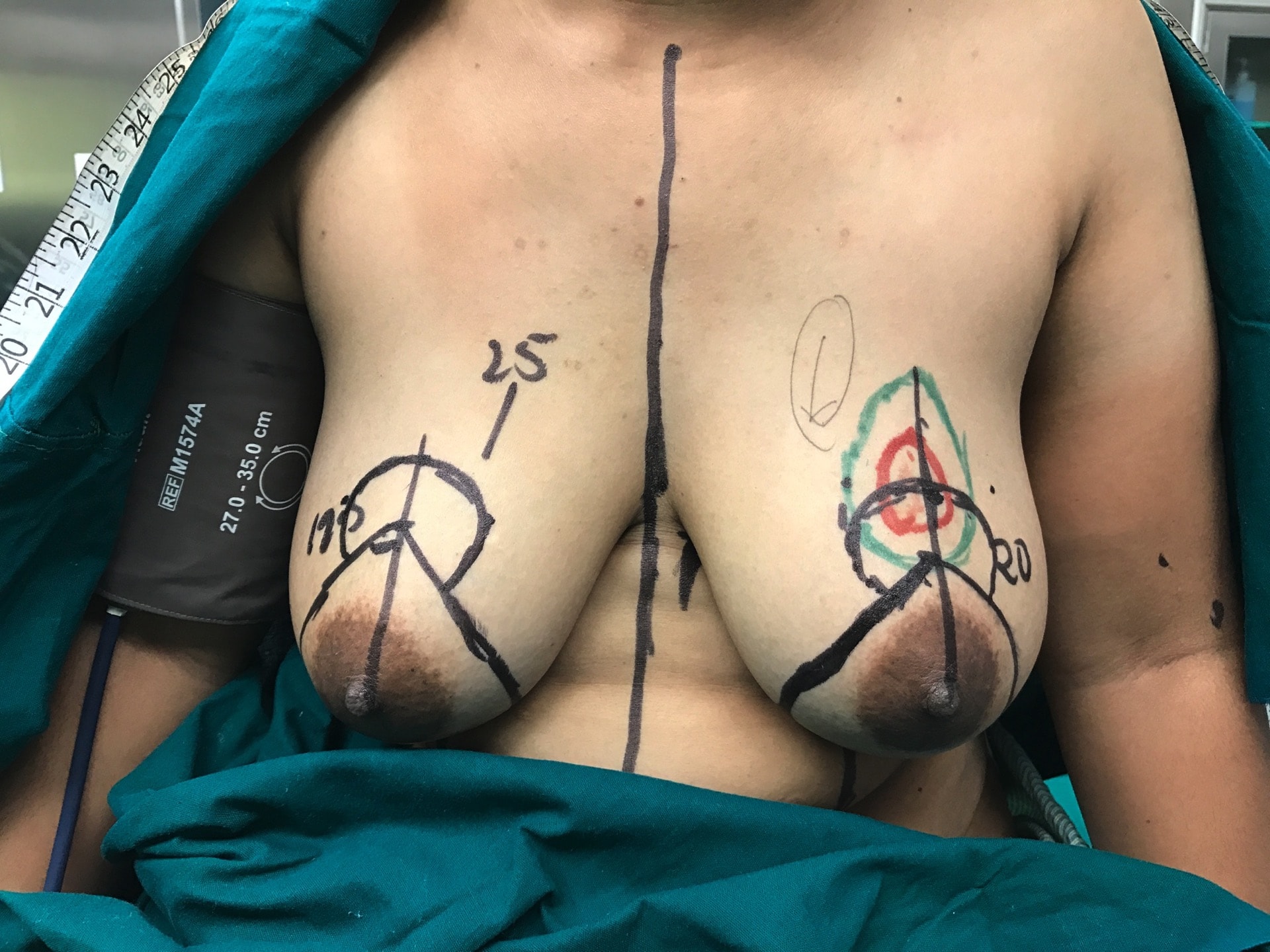
The tumour is in the upper quadrant at 12 o’clock position, 5-6 cms away from Nipple-Areola Complex
Markings are done in such a way that nipple, which is placed at around 25 cms from suprasternal notch, is lifted to around 20 cms and the wise pattern markings are done
The lower segment is de-epithelised completely
The tumour is widely excised by dissecting it on one side and cutting way beyond the edge
Shaved margins are sent for a frozen section
The tumour bed is marked with clips for identification by radiotherapist
The whole of the lower segment including infero-medial, infero-lateral pedicles and inferior pedicle is used to carry the NAC as the breast is not extensively reduced
Lymph node is dissected out and sentinel node is sent for frozen section through the same incision
The NAC on the lower pedicle is transported to fill-up the gap in upper quadrant
Pect Block (local anaesthesia) is given between both the Pectoralis muscles and between Pectoralis Minor and Serratus Anterior
The filler, which is the extension of the lower pedicle, is filled into the gap and the nipple is carried to the appropriate position
The nipple is sutured, first by interrupted sutures and then with continuous sutures
Similarly on the other side, the wise pattern is marked and a formal inferior pedicle is done with reduction to achieve 10% smaller size compared to the other breast
Care is taken to cut perpendicular down to the chest wall
A sliver of tissue is kept on the chest wall to try to preserve the nerves
NAC is carried on the inferior pedicle and the inferior pedicle is fixed to chest wall to prevent bottoming out later on and the two pillars are closed over the inferior pedicle
NAC is sutured and the skin is closed in two layers
Surgical Histopathology Report
Original tumour size – 2.5cm x 2.3cm x 2cm
IDC Grade II
Foci of DCIS solid and comedo type with high grade nuclei
Nodal involvement: 1/6 nodes positive for atypical or malignant cells
Post surgery
On tissue blocks:-
ER/ PR - negative
HER 2 - negative